What Is Pharmacogenetics | An Overview
A quick overview with examples of Pharmacogenomics, including what it is, how it works and the benefits to patients and prescribing doctors.
What is pharmacogenomics (PGx)?
Pharmacogenetics is a field of research that studies how one’s genes affect their response to a medication. Additional factors that can also influence an individuals’ medication response include:
- Age
- Sex
- Organ function
- Other medications
Approximately 15-30%, and in certain cases 95%, of an individuals’ variability in drug response is attributed to genetics alone.
When we use the words “medication response,” this embodies the full spectrum:
- successful response
- no response
- negative response, also known as an adverse drug reaction (ADR).
Pharmacogenomic testing helps practitioners determine their patient’s genetic response to ~50 different medication classes that are under genetic control.
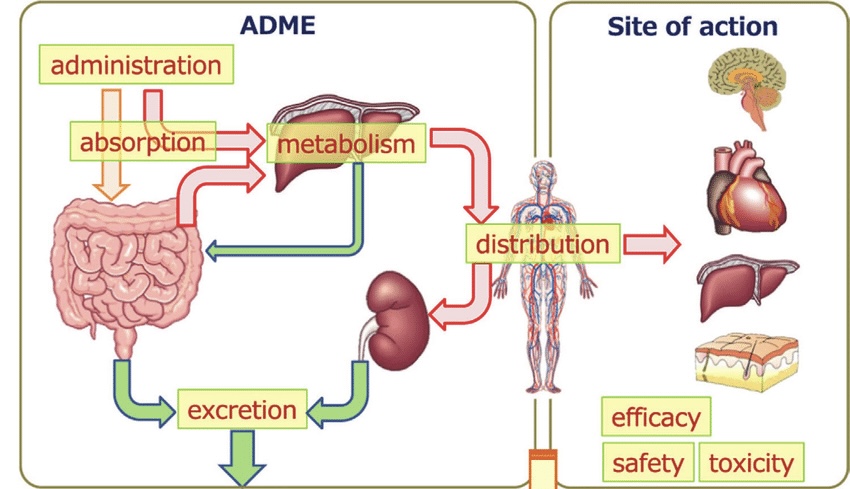
Figure 1.
Through the lens of a tablet/pill
As seen in figure 1, once a medication is ingested, it makes its way through the gut, into the liver, and then into circulation for distribution to multiple organs before excretion in the urine and/or feces. Every tail and point of an arrow in figure 1 is under genetic control and can account for variations in medication response. From the transport proteins that facilitate molecules from tissue to bloodstream and vice versa, to the enzymes that are created in the liver that help breakdown molecules, all have genetic variability and thus are a factor that dictate how long a medication stays in one’s system.
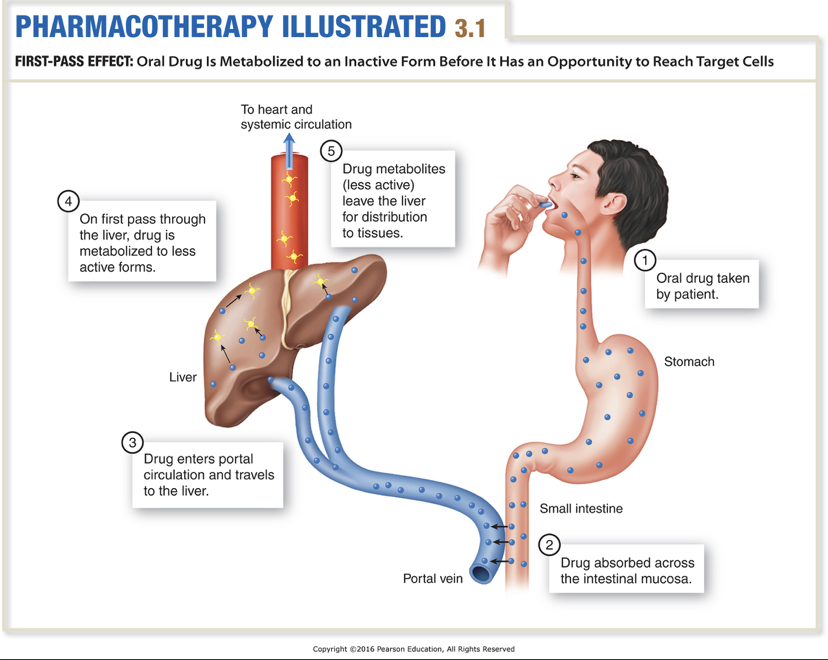
Figure 2.
A closer look at the liver.
The liver acts as a filter for the blood by helping breakdown, or metabolize, any toxins, medications or nutrients which arrive in the stomach/small intestines. Metabolism is facilitated by a family of protein enzymes called cytochrome P450s, which consists of more than 50 different enzymes. Genetic variability exists for these enzymes, creating a spectrum of functionality from “poor-metabolizer” to “rapid-metabolizer.”
Depending on genetics, one may break down a given medication more quickly or slowly, allowing for more of the unchanged molecule to make its way into circulating blood and into other organs. Certain medications are delivered in the “inactive” form which then need to be metabolized by these enzymes for conversion to their “active” form, as we will see in an example to come.
Examples: Opiates, blood-thinners, and stimulants
Opiates like codeine and Tramadol require metabolism by CYP2D6 enzymes in the liver to be converted to their more active form to properly decrease pain. Research has established that those who are CYP2D6 poor metabolizers often experience poorer pain control and might request higher doses of the medication in an effort to manage their pain. On the flipside, those who are rapid metabolizers will have more active opiates in their blood, which can lead to toxicity and could potentially be fatal. As a result, clinical pharmacogenetic guidelines offer excellent suggestions which medications should be avoided by poor and rapid metabolizers.(1).
Clopidogrel is yet another medication that requires metabolism into its active form, but by another liver enzyme CYP2C19. Those who are poor metabolizers are at higher risk for adverse cardiovascular events due to a reduction of blood-thinning (2). Warfarin is another blood thinning agent but does not warrant conversion to its active form. Variations in CYP2C9, a metabolizing enzyme, and VKORC1, an enzyme that activates clotting factors, both play a role in one’s response to warfarin (2).
Lastly, let’s look at genes affecting methylphenidate (Ritalin) response in children. It was found that 5 genes assist in predicting a child’s response: SLC6A2, COMT, ADRA2A, SLC6A3 and DRD4 (3).
Benefits of pharmacogenomic panels
Any individual taking medications would benefit from having a pharmacogenomic profile. Additionally practitioners and patients alike will have greater confidence in medication decisions as pharmacogenomics will assist with:
- Individuals who are on many medications, also known as polypharmacy
- Preventing ADRs caused by gene-drug and drug-drug interactions
- Helping elderly patients avoid duplicate medication therapy or side effects
- Increasing confidence in selected drug therapy regimens
- Increased safety and optimization of drug therapy
To learn more about how PGx can benefit your patients and practice, please take a look here and/or book a free consultation with Dr. Erika Gray.
Sources:
- Crews KR, Monte AA, Huddart R, Caudle KE, Kharasch ED, Gaedigk A, Dunnenberger HM, Leeder JS, Callaghan JT, Samer CF, Klein TE, Haidar CE, Van Driest SL, Ruano G, Sangkuhl K, Cavallari LH, Müller DJ, Prows CA, Nagy M, Somogyi AA, Skaar TC. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin Pharmacol Ther. 2021 Oct;110(4):888-896. doi: 10.1002/cpt.2149. Epub 2021 Feb 9. PMID: 33387367; PMCID: PMC8249478.
- Matey ET, Ragan AK, Oyen LJ, Vitek CR, Aoudia SL, Ragab AK, Fee-Schroeder KC, Black JL, Moyer AM, Nicholson WT, Shrestha S, McAllister TM, Sinnwell JP, Faubion SS, Lazaridis KN. Nine-gene pharmacogenomics profile service: The Mayo Clinic experience. Pharmacogenomics J. 2022 Feb;22(1):69-74. doi: 10.1038/s41397-021-00258-0. Epub 2021 Oct 20. PMID: 34671112.
- Myer NM, Boland JR, Faraone SV. Pharmacogenetics predictors of methylphenidate efficacy in childhood ADHD. Mol Psychiatry. 2018 Sep;23(9):1929-1936. doi: 10.1038/mp.2017.234. Epub 2017 Dec 12. PMID: 29230023; PMCID: PMC7039663.